
Introduction
- Death is inevitable. Death is mourned upon since ages and have gathered attention of many philosophers, saints and scholars. Various definition of death were given by multiple experts and with evolution the definition has also evolved over time.
- It came from a Greek word, ‘Thanatos’=death, and ‘logus’=science.
- Thanatology=branch of medical science that deals with study of death.
- In ancient times, Physician’s definition of death: ‘Sudden stoppage of circulation of blood with consequent cessation of vital functions’.
- Black’s law dictionary (1968 edition): ‘the cessation of life, the ceasing to exist, defined by the physicians as total stoppage of circulation of blood and cessation of animal and vital functions consequent thereupon such as respiration, pulsation etc’.
- Shapiro (1969): ‘the irreversible loss of the properties of living matter’.
- Rentoul and smith (1973): ‘complete and persistent cessation of respiration and circulation
- Over time, these definitions were challenged because they emphasized only on circulation and respiration.
- They were also challenged by 2 recent medical advancement:
- CPR (advanced resuscitation techniques)
- Ventilators (advanced life sustaining equipment)
- Due to these advancements new definition was required
- ‘Death is permanent and irreversible cessation of functions of three interlinked vital systems of the body namely, nervous, circulatory and respiratory system’. the ‘Tripod of life’
- These are called as ‘atria mortis’ death’s portal of entry
- This definition is also considered incomplete because:
- Do not talk about brain death
- Do not recognize the medical advancements
- A model definition was formed by American Bar Association and National conference of commissioners of Uniform state laws:
- “An individual who has sustained either (1) Irreversible cessation of circulatory and respiratory functions or (2) irreversible cessation of all functions of the entire brain including the brainstem, is Dead”.
- Features of model definition
- Complete and elaborative
- Recognizes brain death and cardiorespiratory arrest
- Acknowledges life sustaining aid and equipment
Statutory definitions:
I.Section 46 (IPC): “Death denotes the death of a human being unless the contrary appears from the context”
II.Section 2(b) of registration of Births and Death act 1969: “Permanent disappearance of all evidence of life at any time after live birth has taken place”
Medicolegal importance of death
- Death declaration
- Certification of death
- Disposal of the body
- Organ transplantation
- Presumption of death
Types of death
Generally, there are 2 types of death as mentioned in studied in forensic medicine:
- Somatic
- Cellular death/molecular death
Somatic death:
- Also called as clinical death or systemic death.
- It is permanent and irreversible cessation of so called tripod of life i.e. Nervous system, cardiovascular system and respiratory system.
- Individual cells may not die and respond to certain stimuli.
- Somatic death means demise of the person
- Doctors (RMPs) are entitled to issue a death certificate in case of somatic death
Molecular death:
- It is also called as cellular death
- Cells and tissues start to die in absence of circulation.
- Certain tissues live up to certain time period and then die
- WBCs live up to 12 hours after somatic death
- Muscle cells die within 2 hours of somatic death
- The brain cells die faster
- Tissue needing more circulation dies faster.
The time between somatic death and molecular death is important for
- Disposal of the body
- Transplantation purpose
Brain death
There are three types of brain death
- Cortical brain death
- Brainstem death
- Mixed or whole brain death
Cortical Brain Death
- Also called cerebral brain death or persistent vegetative state.
- All the cerebral functions are lost with severe brain dysfunction
Caused due to:
- Hypoxic insult
- Trauma
- Toxic insult
- The brain stem is intact
- Respiration and circulation are sustained.
- Such cases are not considered dead and are called living cadavers.
- Disconnection of life support is permissible but is difficult in some cases
Brain stem death
- It is considered death of the person
- Respiration, circulation and ascending reticular pathways are arrested permanently.
- The cerebrum may be intact but cut off from the brain stem.
- Transplantation of Human organs act 1994:
“Brainstem death means the stage at which all the functions of the brainstem have permanently and irreversibly ceased and is so certified”
Whole brain death
- Also called mixed brain death
- Combination of cortical brain death and brain stem death
- The brain cells die due to anoxia
- The cerebrum dies first and then the midbrain and brainstem.
Determination of Brain death
Medicolegal aspects:
- Organ transplantation
- Discontinuation of life support
- Determination of time of death for criminal and civil litigations.
Determination of brain stem death
Determination is done under Transplantation of Human Organs Act 1994 certified by board of experts.
The board has following members:
- Registered medical Practioner in-charge of the hospital
- An independent RMP nominated by in charge RMP from names approved
- A neurologist or a neuro-surgeon nominated by RMP from the panel approved
- The RMP treating the person
Diagnosing Criteria
- Patient must be in deep coma, ‘Irreversible structural brainstem damage’
- Exclusion of other causes of coma
- Demonstrating absence of brainstem reflexes
- No spontaneous respiration
- Must be examined by the board of experts twice at an interval of 6 hours
- Brain dead certificate has to be signed by all the members.
Other causes of coma
- Hypothermia (temp below 32.2 degree Celsius)
- CNS Depressants drugs like barbiturates, benzodiazepines etc
- Metabolic and endocrine disturbances
- Intoxication
Role of Brainstem reflexes in diagnosing brainstem death
Absence of following reflexes aids in declaration of brainstem death:
- Absence of pupillary response
- Absence of corneal reflex
- Absence of vestibulo-ocular reflex (caloric response)
- Absence of grimace
- Absence of cough/gag
- Absence of cranial motor nerve response to pain stimuli
- Absence of spontaneous respiration.
Sudden death
“When a person of normal health dies, within 24 hours of onset of symptoms and signs of terminal illness, it is called sudden death”.
- It may or may not be preceded by morbid symptoms
- From medicolegal point of view, it may arise suspicion of foul play.
- Certification of death is not possible just by external examination of the patient.
- If the doctor has not attended the patient within two weeks, it is advisable not to issue a death certificate.
Causes of sudden Natural death
- Cardiovascular: CAD, PDA, ASD, VSD, Aneurysms
- Respiratory: BA, Viral Pneumonia, Obstruction, thrombo-embolism
- CNS: Intra-cranial hemorrhage, cerebral thrombosis, embolism, tumor
- Abdominal: perforated ulcer, hepatic failure, hemorrhagic pancreatitis
- Endocrinal: adrenal hemorrhage, diabetic come, Sheehan’s syndrome
- Iatrogenic: abuse of drugs, sudden withdrawal of Beta blockers
- Miscellaneous: anaphylaxis, malaria, sickle cell crisis
- Special causes in children: COT or SID
- Indeterminate: in decomposed bodies.
*
CAD: Coronary Artery Disease
PDA: Patent Ductus Arteriosus
ASD: Atrial Septal defect
VSD: Ventricular Septal Defect
BA: Bronchial Asthma
SID: Sudden Infant Death
Signs of Death
Signs are the changes in the body following death and can be divided into three phases:
- Immediate signs
- Early signs
- Late signs
Immediate signs
These are the signs in the body that happens immediately after death
It Includes:
- Insensibility and loss of EEG rhythm (cessation of nervous system)
- Cessation of circulation
- Cessation of respiration
Cessation of nervous system:
- Loss of sensation to touch pain and temperature
- Loss of voluntary movements
- Loss of reflexes and the muscles become flaccid
- The pupils are dilated and fixed
- These with loss of EEG rhythm for a continuous period of 5 minutes.
- Signs of brain death as discussed earlier.
Cessation of circulation:
- On palpation the pulsation are absent (radial, brachial, femoral and carotid)
- Absence of heart sounds for continuously 5 minutes
- Auscultation done at the apex of heart in the left fifth intercostal space
- Auscultation is done a few times at short intervals.
- Absence of ECG for continuously 5 minutes.
There are certain tests to assess circulation:
- Diaphanous test
- Magnus test
- Icard’s test: 20% Alkaline dye fluorescence solution injected into dermis or subcutaneous tissue
- Pressure test
Cessation of respiration:
- No visible respiratory movements will be observed
- No respiratory movements will be felt.
- The breath sounds are absent when auscultation is performed
- The absence of breath sounds continuously for 5 minutes is evidence of death
Tests to assess the Respiratory signs of death
- Feather test: In this test a feather is brought near the nostrils of the dead. The feather won’t move in case of death. But when there is ongoing respiration, the movement in the feather can be easily seen.
- Mirror test: A mirror is brought in close contact with nostrils of the body. If there are signs of breathing, vapors are formed on the surface of the mirror and if there is no respiration, no signs of vapor will be seen.
- Winslow’s test: A bowl of water is kept on the chest. If there are waves on the surface of the water, it shows signs of respiratory movements. There will be no movements on water in case of death.
Early signs
The early signs of death can be studied under the following heads:
- Changes in the eyes
- Changes in the skin
- Cooling of the body
Changes in the eye:
- The lustre in the eye is lost due to absence of lacrimation
- Reflexes are lost (pupillary reflexes), pupils becomes dilated and fixed
- Muscle tone is lost (eye ball becomes flaccid)
- Corneal changes: becomes partially hazy and completely hazy after 12 hours
- Drying and desiccation of cornea happens
- Cornea becomes wrinkled with central depression
- Changes of Tache norie sclerotiques: blackish brown discoloration of sclera and conjunctiva
- Initially it becomes yellowish (2-3 hours) and then converts to blackish brown discoloration (2-3 days). Happens when eyes remained opened.
- Loss of ocular tension: normal pressure is 16-23 mmHg. Eyes become sunken
- Pupils are circular but the shape may change due to loss of tone in ciliary muscles.
- Retinal changes: due to arrest of circulation the retinal vessels becomes dotted and gives appearance of, ‘Cattle trucking’
Biochemical changes in the eyes:
- The linear rise in Vitreous potassium levels
- The vitreous Transaminase also rises steadily in the vitreous fluid.
Changes in the skin:
- The skin becomes pale and gives ashy white appearance due to absence of circulation (more prominent in fair skin people)
- Looses its elasticity and skin creases
- Contact flattening is noted with pallor appearance
- Cutis anserina may be observed
Cooling of the body:
- Also known as ‘Algor Mortis’
- Algor=coldness, Mortis=After death
The fall in the body temperature is due to:
- There is no heat production due to loss of metabolic, physical and chemical Activity
- The heat regulatory centres are stopped=constant heat loss till it coincide with environmental temperature.
Heat loss happens from the body by 3 mechanisms
- Conduction
- Convection
- Radiation
Newton’s law and explanation
“Loss of heat from a body is directly proportional to the difference between the surface of the body and the surrounding at a given time”
- It applies to inert body but not cadavers
- Cadavers are composed of bone, fat, muscles, fluids protein etc.
- Thus, the rate of fall of temperature is different in different body parts.
- The surface cools first and then the core body temperature.
- This due to insulation of skin and fat and other tissues.
If we take a curve:
- Inert body gives an exponential curve
- Cadaver gives sigmoid curve with initial phase of plateau
- Initial 3-4 hours = loss of temperature from the surface (plateau)
- For 9-12 hours = loss of core body temperature
- After 16-20 hours, the body reaches the ambient temperature.
Recording of the body temperature:
- Special chemical thermometer is used, “Thanatometer”
- It is 25 cm long with graduation from 0 degree to 50 degree Celsius
- Rectal temperature is taken from 4 inches depth
- Or can also be taken from the Subhepatic region
Practical application:
- The loss of body temperature is much faster in cold or temperate countries
- In tropical countries like India, fall of temperature is slower
- Due to increase in environmental temperature greater than the body temp
- In India the average rate of cooling of body is 0.4 degree C to 0.7 C or 0.5 to 0.7 degree C per hour
- General formula: time since death=normal body temperature(37.2)-rectal temperature, divided by avg rate of fall of temperature per hour (0.6)
Factors affecting cooling of the body
- Atmosphere: The temperature will come down rapidly in cold climatic conditions and vice versa
- Media of disposal: ratio of cooling in water, air and grave is 4:2:1 (Casper’s Dictum)
- Body built: Bodies with more fat stores looses heat more slowly
- Age: Children often looses heat more rapidly due to more surface area of their body corresponding to their size.
- Clothing: Clothing do hampers the process of heat loss. More clothes, less heat loss
- Air movement: Air movement speeds up the process of heat loss
- Position and posture of the body
- Cause of death: death due to septicemia etc is warm even after death
Post-mortem caloricity
- Rise in body temperature in contrast to cooling of the body in dead.
- Observed for first 2 hours
Causes:
Post-mortem glycogenolysis:
- It is a compulsory phenomenon that happens after death.
- In an average adult, post-mortem glycogenolysis produces 140 calories
- Rise in body temperature may be 3.6 degree F or 2 degree Celsius.
Cause of death:
- Infective conditions like bacteraemia, septicaemia
- Sunstroke or pontine hemorrhage (loss of heat regulatory centers)
- Tetanus poisoning due to rise in muscular activity.
Medicolegal importance:
- It is a sign of death
- Time since death can be calculated
- Early cooling delays rigor mortis and retards decomposition
Post mortem Lividity
- Also known as Livor mortis, post-mortem Hypostasis, Vibices, Suggilation, post-mortem staining.
- Definition: “Post-mortem lividity is a purplish blue or reddish blue discoloration due to settling of blood by the gravitational force within the dependent, dilated and toneless small veins and capillaries of rete mucosum”
Formation and spread of Livor Mortis
- After death, there is cessation of circulation
- Blood remains in the blood vessels and capillaries
- In the influence of Gravitational force, blood accumulates in the dependent parts of the body
- The vessels looses tone due to stoppage of CNS.
- If the dead body is left undisturbed, the staining starts in small patches by the end of first hour.
- The small patches later coalesce to form uniform staining
- Uniform staining takes 5-6 hours.
- After 5-6 hours the lividity or hypostasis gets fixed.
- Fixation of Lividity can be checked by blanching sign.
- If blanching is present = non fixed lividity
Fixation of lividity
- If the body is undisturbed, staining gets fixed
- If body is disturbed after the fixation, staining will remain the same with slight change in the color
- There will be no staining in the new area
Causes of Fixation of lividity:
- After lividity, blood cannot be easily pass through the vessels
- By end of staining, rigor mortis is established and the vessels are obliterated
- After rigor mortis, vessels of the new area are also compressed.
- There is diffusion of hemoglobin from haemolysed red cells in the stained areas.
General rule:
- If the blanching happens, staining or lividity is not fixed and the time since death is less than 8 hours.
- If there is no blanching, the time since death is more than 6 hours
Features of Post-mortem Lividity:
- It is an intravascular phenomenon
- Post-mortem lividity happens in the dependent part of the body
- Color of livor mortis varies from red to purple (deoxyhemoglobin)
- The area of the body in direct contact does not stains (contact pallor)
- Antemortem lividity may be present in people with feeble circulation
- Post-mortem lividity happens in internal organs also
- It might confuse with contusion
- Lividity in intestine may confuse with infarction
- It is ruled out by signs of patchy appearance with areas of pallor. (called as vibices)
- Glove and stock lividity:
Happens in case of vertical death (hanging).
Staining will be in hands and feet
This pattern gives appearance of gloves and stockings.
- In case of tight inner clothing, lividity happens in those areas
- It does not appear over scar due to lack of blood vessels.
- In case of drowning the lividity happens over head and upper parts of the body
- Body in flowing water current may not show any lividity
- Contact pallor may give rise to errors
- Tight collars and ornaments may give impression of manual strangulation
- Body lying supine in a crumpled blanket may give impression of bruises of assault.
- Gordon and Shapiro observed that lividity may be formed along the sides of the neck.
- Due to incomplete emptying of the superficial veins.
- This should not be mistaken with bruises.
- The differences between post-mortem lividity and bruises and post-mortem lividity and congestion are given below
| Post Mortem lividity | Bruise |
|---|---|
| Due to engorged vessels showing through the skin | Due to rupture of the vessels either superficial or deep |
| On dependent parts and on front and sides of the neck in supine position | Situated anywhere (at site of blunt force trauma) |
| Margins clearly defined, usually horizontal | Margins are irregular, not horizontal |
| Uniform in color | May be variegated in color |
| No swelling | Swelling |
| No superimposed abrasion | Superimposed abrasion may be present |
| Incision shows few oozing points at the site of severed capillaries | Incision shows extravasated blood staining the surrounding tissues |
| Microscopically, the blood elements are found within the blood vessels and there is no signs of inflammation | Microscopically, the blood elements are found outside the blood vessels and there may be evidence of acute inflammation |
Factors affecting Post Mortem lividity
- Position: position of the body may change how lividity sets in.
- Hemorrhage: hemorrhages can alter the intensity of the lividity
- Anemia: this condition can cause very low intensity of lividity and sometimes difficult to assess
- Complexion: darker complexion body may not show lividity very readily
- Cold storage of the body: cold temperature leads to lividity to occur at a much slower rate.
Color and intensity of the lividity
- Depends on color of blood and mode of death
- Normally: bluish pink and bluish purple afterwards
- In severe Anemia and hemorrhage: very faint
- In asphyxia: purple in color
- Lobar pneumonia: less obvious
- Carbon monoxide poisoning: Bright cherry red
- Cyanide: pink
- Chlorates: chocolate brown
- Phosphorus: dark brown
- Nitrites: red brown
- Hydrogen sulphide: bluish green
- Opiates: almost black
- Exposure to cold: cherry red.
- Septic abortion: greyish brown
Medicolegal importance
- Sign of death
- Time since death may be estimated
- Position of the body can be identified
- The lividity in hands may confuse with cyanosis
- May be confused with congestion
- Cause of death can be identified
- Blood dyscrasias/hemorrhagic spots may confuse with lividity
- Lividity in intestines may confuse with infarction and strangulation
Changes in the muscles
The changes in the muscles are as follows:
1.Primary relaxation or primary flaccidity of the muscles
2.Rigor mortis
3.Secondary relaxation or secondary flaccidity
Primary flaccidity
- Happens immediately after death
- This stage last for 1-2 hours
- Happens with somatic death
- All the voluntary and involuntary muscles relax.
- Jaw drops, pupils dilate, sphincters are relaxed
- May result in incontinence of feces and urine
- Molecular or cellular death has not occurred
- Muscles may still respond to electrical and chemical stimuli
- Tendon reaction or Zasko’s Phenomenon may be present
- Pupils may react to atropine or physostigmine.
- The muscles are still alkaline
Rigor Mortis
- Also known as Cadaveric rigidity
- Rigor = rigidity, Mortis = of death
- Definition: “Rigor mortis is that state of muscles of dead body where they become stiff with some degree of shortening that follows the period of primary relaxation or flaccidity”
- It is stiffening of muscles after death.
- When developed completely, the joints and muscles become stiff and adopt a flexion attitude.
- It indicates molecular and cellular death.
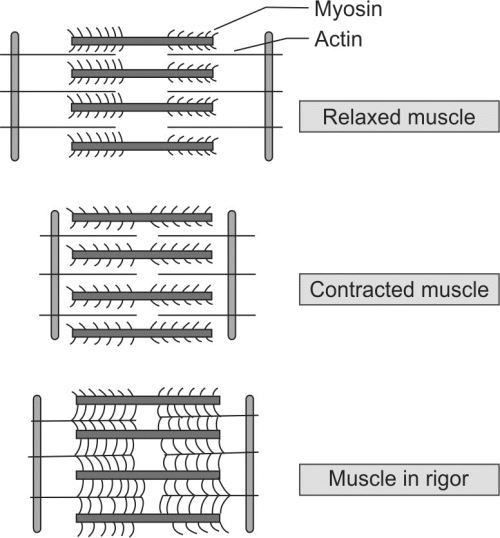
Forensic Anatomy and physiology of muscles
- Each muscle fiber is a single cell (multi-nucleated)
- It is surrounded by sarcolemma
- The muscle fiber is made up of myofibrils
- Myofibrils are made of filaments (thin=actin, thick=myosin)
- Myofibrils are surrounded by sarcoplasmic reticulum.
- The contraction of the muscle depends on
- Actin and myosin
- Tropomyosin and troponin (troponin I, T and C)
Sequence of contraction and relaxation
- Initially there is discharge of motor neuron
- This results in the release of acetylcholine
- Then there is binding of acetylcholine to the receptor
- This sets up an action potential by sodium-potassium pump
- Which leads to depolarization resulting in the release of calcium from sarcoplasmic reticulum
- Calcium binds to troponin C
- This binding exposes the binding site
- The exposure of the receptor site leads to gliding of actin over myosin and formation of cross-linkages
- Ultimately resulting in muscle contraction
Mechanism of Relaxation
For relaxation to happen
- The calcium is pumped back to SR (sarcoplasmic reticulum)
- Then there is cessation of cross linkage between Actin and Myosin
- Relaxation of muscles
For this whole process ATP is required
Mechanism of Rigor mortis
- After somatic death, relaxation is maintained by stored glycogen
- After depletion of glycogen stores ATP drops
- There is formation of actin and myosin complex
- This is a gel like structure that causes rigidity
- This ultimately leads to rigor mortis
- The muscles starts to become acidic due to lactic acid.
- Rigor mortis persist till destruction of protein filaments due to autolysis.
- Rigor mortis can be broken by mechanical force
- If a limb is flexed forcibly, the limb becomes flaccid and remain so.
- It is known as ‘breaking of Rigor mortis’
- Note: Rigor mortis is broken in process of mobilization of body from the crime scene
Onset and disappearance of Rigor mortis:
- It occurs early in involuntary muscles than voluntary muscles
- In involuntary muscles it appears in the heart within an hour after death
- Rigor mortis develops in the following order:
- Muscles of eyelid: 3-4 hours
- Muscles of the face: 4-5 hours
- Neck and trunk: 5-7 hours
- Muscles of upper extremities: 7-9 hours
- Muscles of the leg: 11-12 hours
- In the skin rigor mortis may present as ‘cutis anserina’
- The rigidity passes of in the same order as it started.
- In India rigor mortis starts in 2-3 hours
- Rule of 12: takes 12 hours to develop, remain for 12 and goes in 12
- This is called ‘march of rigor’
Factors influencing Rigor Mortis:
- Age
- Physique of the person
- Season
- Cause of death
- Condition of the muscles


Medicolegal Importance of Rigor Mortis
- It is a sign of death
- Time since death can be estimated
- May be confused with cadaveric spasm
- Breaking of rigor can lead to errors
- It is possible in paralyzed limb also
- Position of the body can be estimated
Differential diagnosis and conditions stimulating Rigor mortis
- Freezing or Cold stiffening
- Heat coagulation or Heat stiffening
- Putrefaction or Gas stiffening
- Cadaveric spasm
Cold stiffening:
- Happens when body is exposed to the freezing temperature
- The tissues become solidified and stiff
- After warming the body, the stiffness goes off and then Rigor sets in.
- In modern mortuary, the body undergo cold stiffening due to solidification of body fat.
Heath coagulation or heat stiffening
- Happens when body is subjected to extreme heat above 70 degree C
- Found in death due to electrocution, falling in hot liquid, burning etc
- The heat coagulates the proteins of the muscles and stiffness happens
- Degree is more severe than normal rigor
- In such cases Normal rigor does not set in.
- The body adopts a Pugilistic attitude. Attitude of a boxer.
- The stiffness will persist till putrefaction or decomposition.
Putrefaction or gas stiffening:
- Stiffening happens due to accumulation of putrefactive gases
- Causes false rigidity
- Limbs will be stiff even without support.
- Found in decomposed bodies.
Cadaveric spasm:
- Also called instantaneous rigor, instant rigor, cataleptic rigidity
- “Cadaveric spasm is a state where muscles or group of muscles, instead of going under primary relaxation after death, go into a sudden state of stiffening”.
- This is a rare condition
Conditions necessary for its development:
- Somatic death must occur with extreme rapidity
- Person under emotional tension
- Muscles must be in physical activity
- In cadaveric spasm certain group of muscles do not undergo primary relaxation.
- It involves only certain group of muscles
- Body may be found holding a knife, a gun or hair (in homicide) or weeds or grass in case of drowning.
- Such findings are not found in rigor mortis
- The cadaveric spasm is more pronounced than rigor mortis.
- It can be broken only due to putrefaction.
Medico-legal importance:
- It indicates sudden death associated with emotional tension
- It indicates the muscles in physical activity
- It may indicates nature of death.
Secondary Relaxation
- It involves secondary relaxation of muscles followed by rigor mortis
- Muscles become flaccid and soft. The muscle reaction is alkaline
- There is no response to mechanical, electrical or chemical stimuli
Difference between Rigor mortis and heat stiffening:
| Features | Rigor Mortis | Heat stiffening |
|---|---|---|
| Nature | Post mortem | May be antemortem or post mortem |
| Degree of Stiffness | Comparatively moderate | Comparatively high |
| Mechanism | Breakdown of ATP | Due to coagulation of muscles |
| Associated features | Nothing specific | Signs of exposure to heat will be present like blisters, burning, heat ruptures etc. |
Difference between Rigor mortis and cadaveric spasm:
| Features | Rigor mortis | Cadaveric spasm |
|---|---|---|
| Time of onset | 1-2 hours after death | Immediate |
| Muscles involved | All muscles are involved | Usually group of muscles like hand |
| Degree of stiffness | Comparatively moderate | Comparatively strong |
| Predisposing factors | None | Excitement, fear, emotional disturbance |
| Mechanism | Breakdown of ATP | Not known |
| Medicolegal importance | Helps to know time since death, position of the body | Helps to suggest manner of death |